



The evolution and application of vapocoolant sprays in myofascial trigger point therapy
A historical review of vapocoolant sprays used in the "spray and stretch" technique, then and now.
By Janet Travell Street
The use of vapocoolant sprays for myofascial trigger point therapy represents a convergence of medical innovation, environmental science, and clinical pragmatism. Developed through decades of research, these sprays have become indispensable tools for pain management, particularly in the treatment of musculoskeletal disorders. This paper explores the historical trajectory of vapocoolant sprays, their formulation challenges, and their therapeutic mechanisms, while proposing advancements for modern clinical practice.
Early Foundations: Hans Kraus and the Birth of Spray and Stretch
The origins of the "spray and stretch" technique can be traced to Dr. Hans Kraus, an Austrian-American physiatrist who pioneered its use in the 1940s. Kraus, known for his work with circus performers and athletes, first employed ethyl chloride spray to rapidly cool muscles during stretching exercises.
Kraus’s approach aimed to alleviate acute muscle spasms by combining cryotherapy with passive stretching, a method he termed "thermal shock". Kraus’s technique capitalized on ethyl chloride’s rapid evaporation, which temporarily numbed the skin and underlying tissues, enabling deeper mechanical manipulation of hypertonic muscles.1 Kraus’s methodology emphasized selective trigger point injections followed by therapeutic exercise rather than repetitive pharmacologic interventions. His insistence on comprehensive rehabilitation programs—integrating strength training, flexibility exercises, and postural correction—laid the groundwork for modern physiatry.
Janet Travell and Presidential Validation
Dr. Janet Travell, who became President John F. Kennedy’s personal physician, first learned of Kraus’s “treatment of joint sprains and muscle injuries with ethyl chloride spray, which he described as surface anesthesia for relief of painful motion,”2 and expanded on Kraus’s work in the 1950s. In the summer of 1961, Travell asked Kraus to see President Kennedy and create an individualized exercise program to help with Kennedy’s back pain relief, which included swimming, therapeutic exercises and massage.3
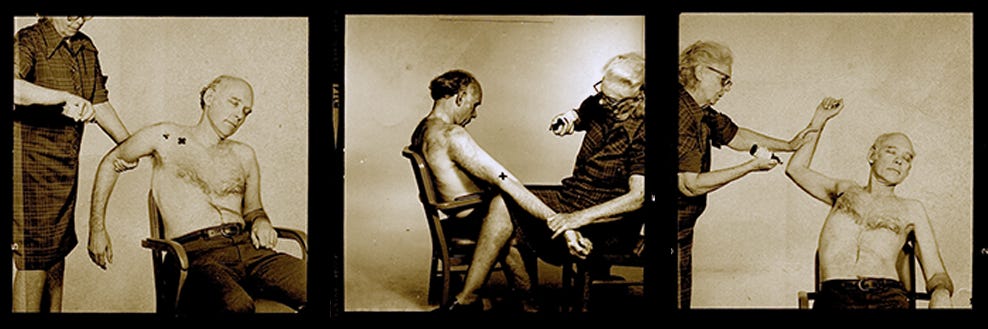
Travell’s spray and stretch technique utilized ethyl chloride spray to treat Kennedy’s chronic back pain and post-surgical knee stiffness, documenting dramatic improvements in his range of motion. Her application involved spraying the skin over trigger points while passively stretching the affected muscles, a technique she popularized through clinical demonstrations. Travell’s contributions extended to codifying diagnostic criteria for myofascial trigger points, including palpable taut bands, referred pain patterns, and localized tenderness.4
Janet Travell and Charles L. Gebauer
In her 1968 autobiography, Janet Travell wrote:
I knew that when used locally for muscular pain, ethyl chloride was acting not as a drug, but only as cold in a bottle — a physical agent in a pharmacological package. I wanted to find a safe nontoxic substitute with comparable cooling effects for medical use in the relief of pain.
One day, my secretary in the office at 9 West 16th Street interrupted me when I was with a patient.
“There’s a man from a drug company who wants to talk with you about . . .”
“Tell him I’m sorry, I haven’t time,” I cut her short.
Presently she returned. “The gentleman is still here. He’s been waiting an hour.”
“What gentleman?” I asked.
“It’s Mr. Gebauer, president of the company that makes all that ethyl chloride you buy.”
Mr. Charles L. Gebauer and I became friends. He was a chemist who had an altruistic view of life and some fifty years’ experience with manufacturing and marketing ethyl chloride for prescription use. He wanted to know what I was doing with so much of his product and he became interested in my search for an ideal vapocoolant spray. In 1951, when I attended a meeting at the Federation of American Societies for Experimental Biology on Cleveland, Ohio, I visited a chemical plant there. The fine glass nozzles of the ethyl chloride spray bottles were drawn from heated glass tubing and calibrated by hand; it was an unusual craft.
That day I persuaded Mr. Gabauer to make a modest grant to Cornell University medical College in support of my research in the Department of Pharmacology on how cold sprays acted to relieve pain. With the money, I obtained an eight-channel Speedomax . . . ‘Max’ enabled me to measure objectively some physiological effects of volatile mixtures of halogenated hydrocarbons that cooled by rapid evaporation at body temperatures . . . They were known to be nonflammable, nonexplosive, and virtually nontoxic. For the purpose of relieving pain associated with myofascial trigger mechanism, the kind of nozzle was important, we found. The nozzle-opener had also to be handy to operate, and it ought not to drip the spray liquid on the fingers or they might become frozen.5
Eventually, the Gebauer Chemical Company marketed for medical distribution the mixture I had selected, dispensed in a handy bottle with a satisfactory calibrated spray nozzle. 6
Gebauer’s product Janet Travell describes was called Fluori-Methane, which was later replaced by Spray and Stretch®.
In 1990, Travell, Simons and Simons published a paper entitled, “Protecting the Ozone Layer,”7 which addressed their concerns over the use of vapocoolant sprays and potential environmental hazards.
Gebauer Company: Pioneering Legacy in Vapocoolants
In 1898, brothers Charles and Theophil Gebauer founded the Gebauer Company. Their first product, Gebauer’s Ethyl Chloride®, was the most widely used local anesthetic until 1905, when a German chemist introduced Novocain®.
In 1901, Charles Gebauer developed one of the earliest aerosol containers to be commercially marketed. This innovative resealable metal tube allowed for jet stream dispension of Gebauer’s Ethyl Chloride®, revolutionizing the product’s use.
Founded in 1898 by brothers Charles and Theophil Gebauer in Cleveland, Ohio
In 1901, Charles patented a metal tube that dispensed ethyl chloride in a jet stream
Gebauer's Ethyl Chloride was the primary local anesthetic used in 1902
Supplied ethyl chloride to the armed forces during World War I and II
The Rose family acquired Gebauer in the 1960s8
Formulation Challenges: From Ethyl Chloride to Modern Alternatives
Gebauer’s Ethyl Chloride, introduced in 1901, became the gold standard for vapocoolants due to its rapid cooling effect (−20°C upon evaporation) and immediate analgesic properties. Clinically, it proved effective for venipuncture, minor surgeries, and sports injuries.9
Transition to Safer Alternatives: Fluoromethane and HFCs
The 1987 Montreal Protocol accelerated the shift toward environmentally friendly refrigerants. Gebauer introduced fluoromethane (1,1,1,3,3-pentafluoropropane/1,1,1,2-tetrafluoroethane) sprays, which offered comparable cooling (−11°C to 4°C) without flammability. These hydrofluorocarbons (HFCs) had negligible ozone depletion potential.
Where to Buy
Gebauer’s vapocoolant products are available through distributors on their website.
Ethyl Chloride® ACCU-STREAM™ 360™ with Sure Lock Technology™
This new packaging is currently available as a Medium Stream (#0386-0001-11) and a Fine Stream (#0386-0001-13). For customers that have been using Gebauer’s Ethyl Chloride Medium Stream 3.5 Fl Oz (103.5 ml) Aerosol Can (#0386-0001-06) please note that this product has been discontinued, replaced by Gebauer’s Ethyl Chloride Accu-Stream 360 Medium Stream, 3.5 Fl Oz (103.5ml) (#0386-0001-11)
Gebauer’s Spray and Stretch®
Gebauer introduced Spray and Stretch®, an instant topical anesthetic skin refrigerant that effectively manages myofascial pain and trigger point release when used in conjunction with the spray and stretch technique. Spray and Stretch® is also indicated for treating muscle spasms, restricted motion, and minor sports injuries. Spray and Stretch® is a prescription medical device available to licensed healthcare practitioners.
Gebauer’s Spray and Stretch® remains a cornerstone in trigger point therapy since its introduction in the mid-20th century. As a prescription medical device, it utilizes a non-flammable, non-ozone-depleting formula (1,1,1,3,3-pentafluoropropane/1,1,1,2-tetrafluoroethane) to achieve rapid cooling (−11°C to 4°C). Clinicians favor its fine-stream spray for precise application during the "spray and stretch" technique, which reduces pain perception and facilitates muscle elongation.
Using Ice as a Cryotherapeutic Agent vs. Vapocoolant Sprays in Spray and Stretch Therapy
Cryostretch and cryokinetics refers to the use of cryotherapy to facilitate joint movement. Decreasing pain and muscle guarding may lead to improved flexibility and muscle function. An additional method of cryotherapy involves the use of vapocoolant sprays (fluori-methane and ethyl chloride), which provide very effective cutaneous local anesthesia and are commonly used to treat myofascial trigger points. The use of cryotherapy in this context promotes normal muscle resting length by a ‘spray and stretch’ technique rather than by cooling the muscle itself.10
Pros
Inexpensive and widely available, requiring no specialized equipment or prescriptions.
No regulatory restrictions, making it accessible to practitioners in regions with licensing barriers.
No risk of flammability, toxicity, or ozone depletion, unlike older vapocoolants.
Minimal risk of chemical irritation or allergic reactions.
Reduces swelling via vasoconstriction and lowers tissue metabolism.
Effective for acute injuries and post-stretch cooling to maintain tissue elongation.
Cons
Requires time-intensive techniques (e.g., ice massage) and lacks precision for targeting trigger points.
Cooling is slower compared to vapocoolants, potentially delaying pain relief during stretching.
Moisture from melting ice complicates application and may reduce patient comfort.
Temporary reduction in muscle function and range of motion if applied pre-activity.
Prolonged application (>20 minutes) can cause frostbite or nerve damage.
Learning the Spray and Stretch technique today
The Spray and Stretch technique is described in detail in Travell, Simons & Simons' Myofascial Pain and Dysfunction: The Trigger Point Manuals. While the third edition consolidates previous volumes and emphasizes newer evidence-based approaches, it retains foundational techniques like Spray and Stretch. Earlier editions (1st and 2nd) explicitly included Spray and Stretch as a core method for myofascial trigger point therapy.
In the video series, “Myofascial Pain Syndromes: The Travell Trigger Point Tapes,” practitioners can study Janet Travell’s Spray and Stretch technique, as part of her entire treatment protocol.
Clinical Demand for Myofascial Trigger Point Therapy
The global myofascial pain syndrome market, projected to grow at 2.75% CAGR (2025–2035), fuels innovation.11 Key factors include:
Aging Populations: 23% of adults over 65 report chronic musculoskeletal pain, necessitating non-invasive therapies like spray and stretch.
Shift to Outpatient Care: 68% of physical therapists now incorporate vapocoolants for in-office trigger point release, avoiding costly hospital referrals.
Conclusion
Today’s myofascial trigger point therapists depend on the availability of vapocoolant products designed for the Spray and Stretch technique. Stretch without spray is often used due to a lack of access to vapocoolant products or a lack of understanding of the benefits of using the Spray and Stretch technique.
Janet Travell’s Spray and Stretch technique can be learned through studying the Travell and Simons’ Myofascial Pain and Dysfunction: The Trigger Point Manuals, by watching Myofascial Pain Syndromes: The Travell Trigger Point Tapes video series, and by attending in-person workshops with trigger point therapy “cold spray” or “spray and stretch” experts.
Future innovations should prioritize biodegradable propellants and cost-reduction strategies to bridge this gap. Ice remains a viable, low-cost alternative for practitioners restricted by licensing or cost barriers, though it is less efficient for rapid trigger point therapy.
References
Kraus H. The use of surface anesthesia in the treatment of painful motion. JAMA. 1941;116(27):2582-7.
Travell JG. Office hours: day and night. New York: World Publishing Company; 1968. p. 261-2.
Travell JG. Office hours: day and night. New York: World Publishing Company; 1968. p. 388.
Travell JG, Simons DG. Myofascial pain and dysfunction: the trigger point manual. Volume 1, Upper half of body. 2nd ed. Baltimore: Williams & Wilkins; 1999.
Travell JG. Office hours: day and night. New York: World Publishing Company; 1968. p. 275-276.
Simons DG, Travell JG, Simons LS. Protecting the ozone layer. Arch Phys Med Rehabil. 1990;71(1):64. PMID: 2297313.